
Facilitator's notes
The Dartmouth Institute (TDI) and the Institute for Healthcare Improvement (IHI) organized a community of senior leaders to discover how “the coproduction of healthcare service” might contribute to work on the strategic priorities of their organizations.
The following organizations participated regularly:
- Bellin Health, Green Bay, WI, USA
- Cambridge Health Alliance, Boston, MA, USA
- Cleveland Metro General Hospital, Cleveland, OH, USA
- Dartmouth Hitchcock Health System, Lebanon, NH, USA
- East London NHS Trust, London, GBR
- Eastern Health, Melbourne, AUS
- Einstein Medical Center, Sao Paulo, BRA
- Region Jönköping, Jönköping, SWE
- Royal Free Infirmary, London, GBR
After discussions with several organizations and further clarification of the aim of a learning community, we formed a shared aim:
Discover, explore & collate ways of implementing system strategic plans in diverse settings by the redesign of service where professionals and patients meet, using a “coproduction” lens.
We met initially & every six months in a face-to-face session and subsequently in monthly virtual sessions facilitated by use of a “zoom” platform that made it easy for participants across the world to participate. Our total time together spanned approximately 18 months.
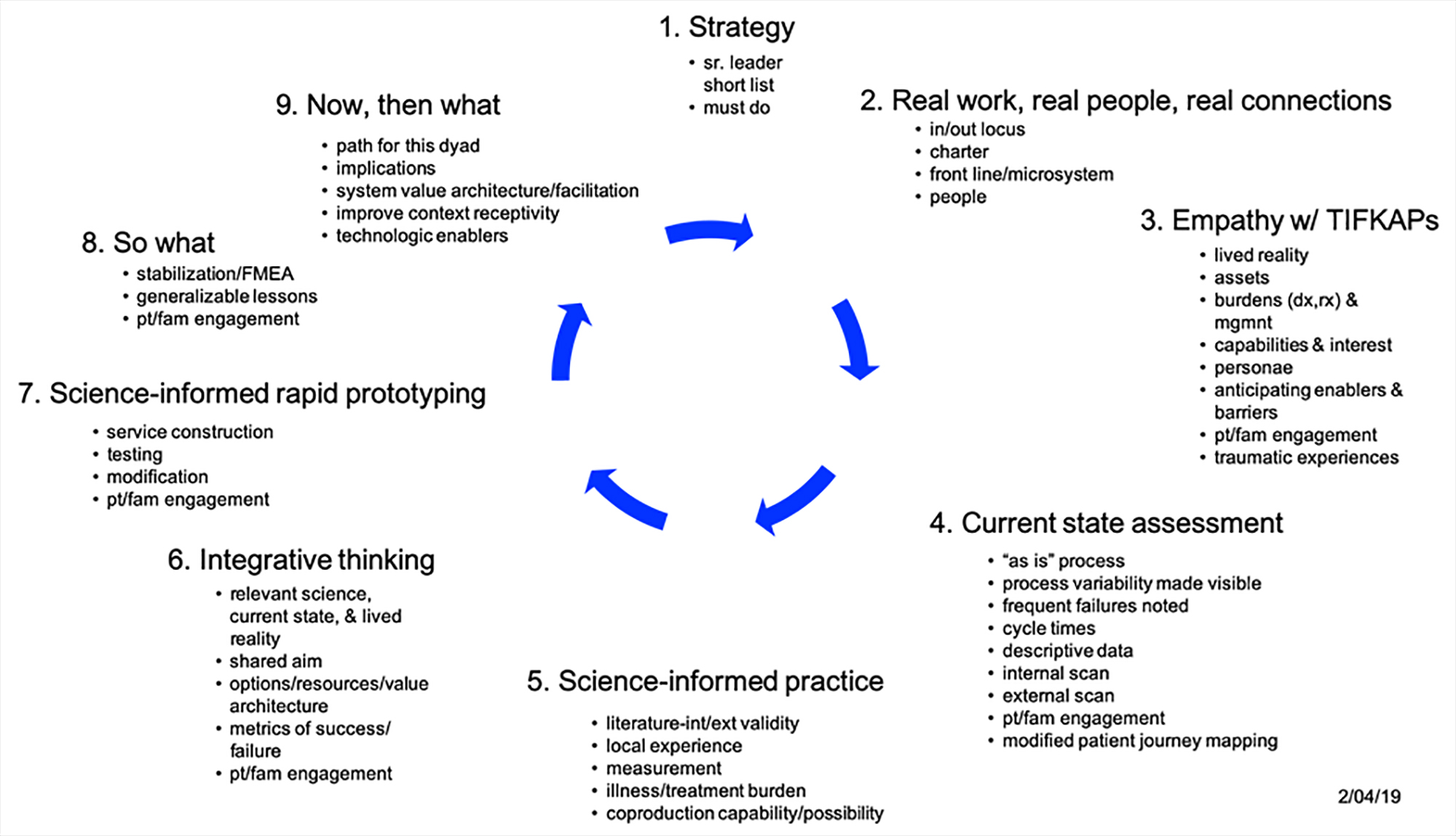
To facilitate our work, we created a learning plan jpg, 508.1 kB. for our time together. We began by identifying, clarifying the strategically important areas in the organizations. We connected the “front line” work microsystems where the people sometimes known as professionals and the people sometimes known as “patients” connected. We sought to develop an empathic understanding of “The Individuals Formerly Known As Patients” (TIFKAP). We developed “personae” that helped the subpopulation of TIFKAPs come alive. We explored the current state of the system that needed to be navigated in the experience of patients and families as they sought help. Then we turned our attention to how our empathic understanding of those sometimes known as patients, our insights into the current state of the system needing navigation, and the literature of the science-informed practices that were relevant. This integrative step involved bridging the different ways in which these knowledge domains were developed & used. Subsequently (as well as along the way) we created prototypes of change which could be tested. We assessed what had been learned, what might need to be done to use these insights throughout the organizations involved.
{kind=link}
As we moved around the cycle of learning, a variety of experts were identified and we invited them to introduce us to their thinking. They included:
- Victor Montori – Professor, Mayo Clinic
- Kasey Boehmer – Assistant Professor, Mayo Clinic
- Roger Martin – Consultant; formerly Dean, Rotman School of Management
- Jennifer Riel – Strategist, Ideo; formerly adjunct faculty, Rotman School of Management
- Glenn Robert – Professor, King’s College, UK
- Glyn Elwyn – Professor, TDI
- Gene Nelson – Professor, TDI
- Rachel Thompson – Senior Research Fellow, University of Sydney; formerly Assistant Professor, TDI
- Estee Neuwirth – Senior Director, Kaiser Permanente
- Maureen Bisognano – President Emerita and Senior Fellow, IHI
- Gouri Gupte – Director of Performance Improvement, CHA
- Catherine Dale – Programme Director for Patient Safety, NHS Health Innovation Network
- Julie Johnson – Professor, Feinberg School of Medicine
- John Whittington – Senior Fellow, IHI
Among the lessons we took away were these:
- Top leaders’ short, focused list not always so clear and there were “non-stop” additions to the related activities [of the designated learning project] can emerge.
- ‘Improvement’ templates for chartering a local project are often agnostic re: patients’ lived reality, experiences of navigating the current “as is” system.
- Sharper insights into the underlying epistemology of coproduction, and relevant learning approaches:
- Building insight into the lived reality, aims of those we sometimes call “patients” can occur in many ways
- Key to using that insight is a summary, persona description, etc.
- Current state of the system often stops short of mapping the experience, feelings of those we call “patients” as they experience the “as is” journey in the system
- In our rush to label our knowledge as ‘evidence-based’ we overlook the gaps in our science-informed thinking…and we stop short of summarizing, synthesizing what we know and its limitations
- We are not in the habit of linking, integrating our knowledge of the lived reality of TIFKAPs, of the ‘as-is’ system current state and of the science-informed practices when we undertake improvement efforts
- Our tools, such as a process flow chart, may inadvertently reinforce a ‘product-making’ logic
- Zoom-enabled discussions work better in groups of about 5-8, important to use break-out rooms which are best ‘assigned’ ahead of time
- Many “branching”, “connecting” opportunities present themselves, zoom sessions enable them. Some follow-on work best done in subgroups
- Current measurement & professional education/development efforts not yet very helpful
A working bibliography helped us and is appended.
For the facilitating team:
Paul Batalden
Rachel Forcino
Joy McAvoy